



























Patient 16

View More Photos of this Patient
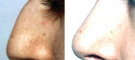
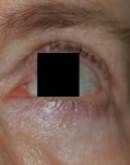
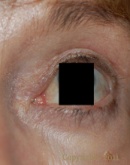
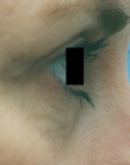
This 45 year-old hispanic female with thyroid ophthalmopathy (bulging eyes) wished to smooth out the lower lids and make the eye appear more “normal.” She did not want to have a more invasive surgery to drop the eye deeper and lower into the bony orbit.
Patient 17


View More Photos of this Patient
This 61 year-old female wished to rejuvenate her upper eyelids. Since she wore glasses, her lower lids did not bother her.
Patient 18

View More Photos of this Patient
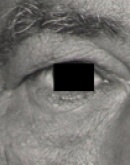
This 59 year-old Hispanic gentleman had upper lid excess skin that caused lid droop, difficulty with upward gaze, and easy fatigue with reading. His ophthalmologist recommended functional and aesthetic blepharoplasty and repair of lid droop.
Patient 19


View More Photos of this Patient
This 42 year-old female wished to rejuvenate her upper eyelids to be competitive with her younger colleagues.
Patient 20


View More Photos of this Patient
This 51 year-old female wished to have upper eyelid surgery to refresh her appearance and gain a competitive edge in the workplace.
Patient 21


View More Photos of this Patient
This 60 year-old female wanted to have upper eyelid surgery to remove the excess skin from her upper lids and get rid of drooping.
Patient 22

View More Photos of this Patient
This 48 year-old wished to have eyelid rejuvenation.
Patient 23


View More Photos of this Patient
This 55 year-old Hispanic woman wished to rejuvenate both her upper and lower eyelids.
Patient 24


View More Photos of this Patient
This 42 year-old female wished to rejuvenate her upper eyelids to be competitive with her younger colleagues.
Patient 25


View More Photos of this Patient
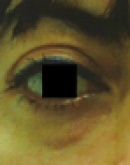
This 36 year-old female wished to remove the dark circles under her eyes without surgery.
Patient 26
View More Photos of this Patient
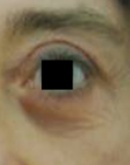
This 68 year-old female had eyelid surgery when she was in her 20’s but wanted revision surgery to remove the fullness near the corners of her upper eyelids. In addition, she wanted to get rid of the left lower lid bag. Because of her past history of Bell’s Palsy, and a prior resection of right lower eyelid skin for cancer, she had some resultant asymmetry. She wanted to attain more symmetry.
Patient 27


View More Photos of this Patient
This 56 year-old female wished to rejuvenate her eyelids. She felt that the excess upper eyelid skin made her look tired.
Patient 28

View More Photos of this Patient
This 52 year-old female wanted to rejuvenate her upper lids. She didn’t like that the skin hung onto the lash line and made it hard for her to apply her makeup. She also didn’t like that the excess skin covered the lower part of her upper eyelid.
Patient 29


View More Photos of this Patient
This 69 year-old female had a complicated past medical history that contributed to her lid droop. First, she had a tumor removed from the front of her skull that left her with a bony depression in her forehead. During the surgery to remove the tumor and repair the bony defect, there was an injury to the nerve that stimulates the elevation of the brow muscle. An ophthalmologist mistakenly attributed the drooping to excess upper eyelid skin, and performed a blepharoplasty to remove some skin. In fact, the problem was not extra eyelid skin, but a drop in brow position. When I saw this patient in consultation, I recommended direct brow lift surgery to restore proper brow position.
Patient 30


View More Photos of this Patient
This 39 year-old female wanted upper eyelid rejuvenation to remain competitive in the workforce.